Discussion
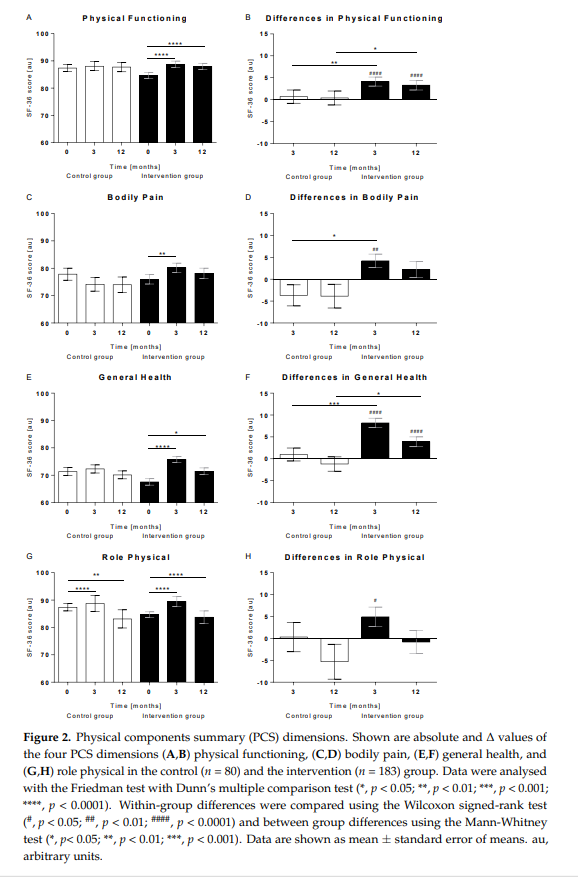
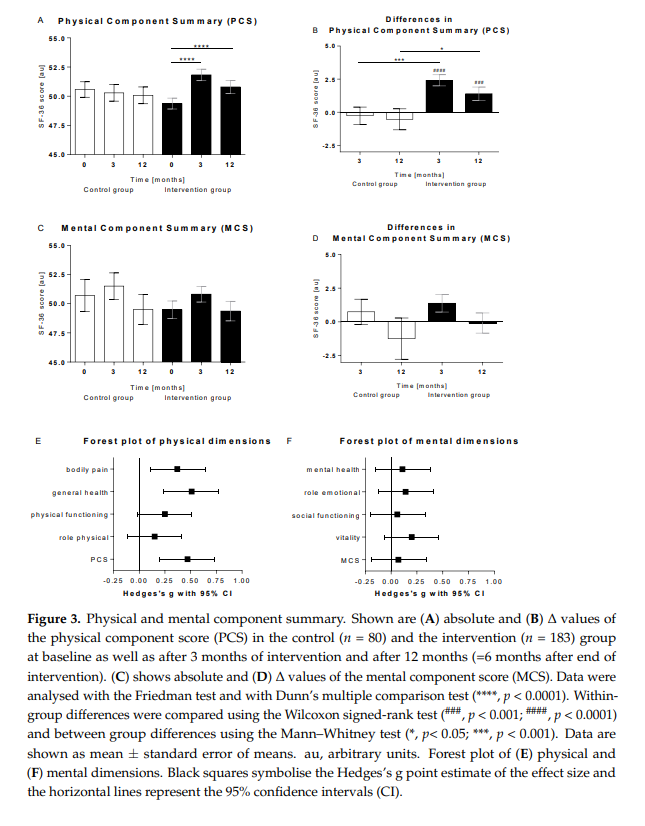
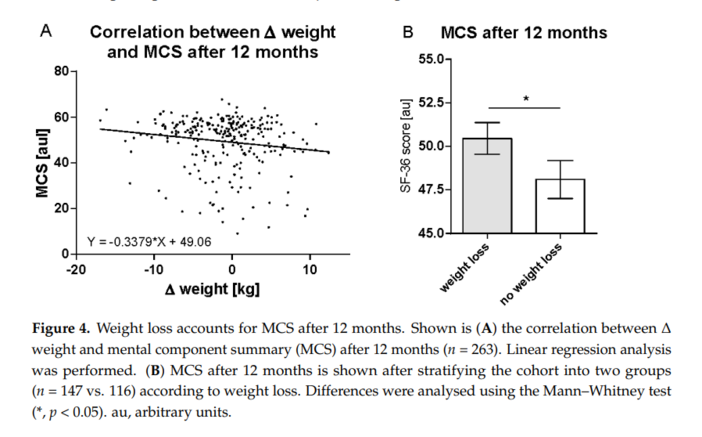
In the international, multicentre, randomised-controlled ACOORH trial, a high-protein, low-glycaemic, meal replacement-based lifestyle intervention was more effective in improving HRQOL than a control lifestyle intervention alone. The improvement of PCS and all individual items of the PCS were significantly more pronounced in the intervention group, whereas higher weight loss was generally associated with higher values of MCS.
So far, we can demonstrate that starting a lifestyle intervention accompanied by high-protein, low-glycaemic meal replacement for overweight or obese persons with at least one criterion of the metabolic syndrome reduced body weight more effectively compared to controls with an ETD of −3.2 kg [−4.0; −2.5] and was able to maintain weight loss long-term [6]. These effects were accompanied by significantly stronger improvements in blood pressure [10]. Individuals with prediabetes also benefited more, since significantly more participants of the intervention group (50 vs. 31%) converted to normoglycemia [7]. Meal-replacement and accompanying nutrition counselling also seem to have influenced nutritional behaviour long term, since there was a decrease in daily carbohydrate consumption but a significant increase in dietary protein in the intervention group [8]. Moreover, significantly higher reductions in insulin, leptin, and inflammation markers were observed, which might explain why it was easier for the participants of the intervention group to lose weight [9,11]. However, all those improvements in clinical and laboratory parameters would be useless if participants would feel worse during the intervention, and replacing meals with a liquid meal replacement might have the potential to negatively impact quality of life.
However, having to go without solid food and using meal replacement for a period of time does not appear to negatively affect patients’ well-being, since the improvements in PCS and MCS were higher during the meal replacement phase compared to the follow -up phase. Participants seem to be able to endure the meal replacement well if they experience weight loss in return [14,15]. A current meta-analysis of Marcos-Delgado et al. [16] has shown that lifestyle interventions have the potential to improve HRQOL, but not all types of intervention appear to be equally effective. With Hedges’ g [95% confidence interval] standardised effect size of 0.47 [0.20; 0.73], our results for the overall effect in physical dimensions were perfectly in line with the reported meta-analysis data of 0.60 [0.31; 0.88], not only with respect to the overall effect size in PCS of but also with the expected effects on the individual dimensions. Thus, the strongest improvements can be seen for general health, followed by bodily pain, and the lowest effects for physical functioning and role-physical. Thus, our findings confirm earlier reports demonstrating beneficial effects of the used meal replacement on HRQOL measured by SF-36. In obese females as well as in overweight type 2 diabetes, patients’ weight loss and increase in HRQOL were more pronounced in the groups with the meal replacement-based lifestyle intervention [17,18]. In the latter, the observed effects on HRQOL were stronger for the PCS than for MCS, too [18]. Therefore, it could be speculated that bioactive components of the meal replacement might positively affect physical dimensions of HRQOL [19].
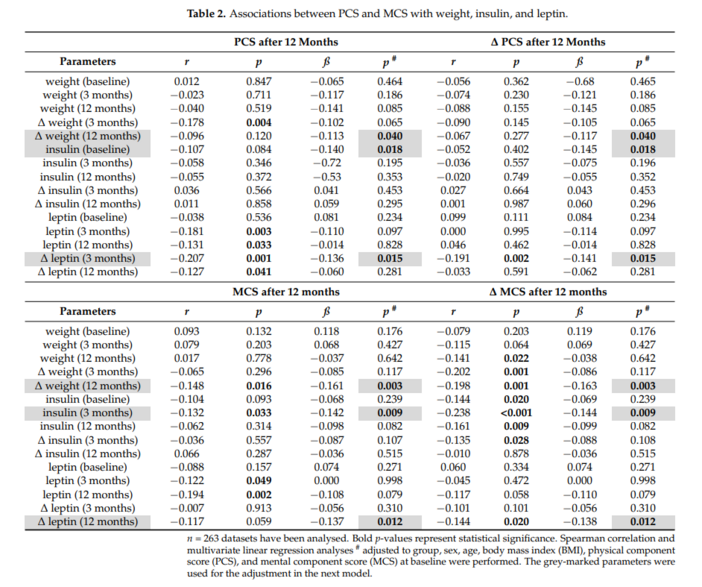
The connection between weight loss achieved and the improvement in MCS seems easy to explain. The predictive value of lower insulin levels (after 3 months) for the higher mental HRQOL after 12 months is less obvious. However, its potential role in the pathogenesis of depression [20] and the positive association of hyperinsulinemia with depression [21] support the correlation between lower insulin levels and higher MCS. In addition, we were able to show in advance that low insulin levels predict a higher success in weight loss [9]. Therefore, the insulin levels are closely linked to the change of weight. Although conflicting results have been reported for the correlation between leptin and depression [22], lifestyle intervention programs have shown that decreasing leptin levels predicted amelioration in depression symptoms independent of changes in body mass or fat mass [23] and improvement of MCS in metabolic syndrome [24].
Several limitations and strengths of our analysis need to be mentioned. As always with the analysis of questionnaires, it can be pointed out that the data are based on self-reports and were not measured objectively. However, the SF-36 is the most commonly used and one of the best-validated questionnaires for determining HRQOL [16] and is particularly useful in comparing HRQOL across diseases, health conditions, or populations. Thus, the results might be meaningful for people at increased risk for the metabolic syndrome, and obesity-specific quality-of-life measures might be particularly useful, e.g., for prediction of long-term compliance. Conducting research applying such obesity-specific HRQOL measures to examine further the meal replacement-based lifestyle intervention’s health effects might be promising in the future.
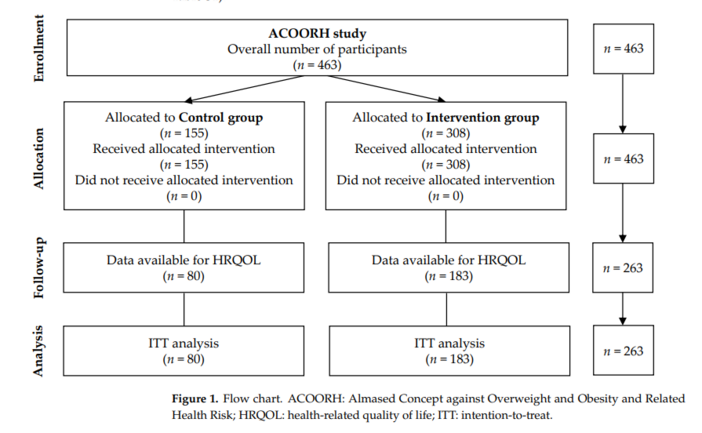
The results might further be limited by the fact that HRQOL data have been available from only 263 out of 463 participants. One explanation for this high missing rate is that the SF-36 questionnaire has only been used in the study centres in Germany and Austria. Additionally, SF-36 data were missing from participants who dropped out and did not come to the final study visit. Indeed, it can be assumed that those people who could not keep up with the lifestyle intervention were more likely to drop out early; therefore, the study results could have been biased and the improvement in quality of life overestimated. However, since the dropout rate in the control group was higher than in the intervention group, this would rather lead to an underestimation of the estimated treatment difference. Another criticism could be that individual missing values were replaced by LOCF. This conservative type of imputation method basically assumes that there are minimal changes over time for the missing data. Thus, the analysis might have led to biased and rather underestimated within-group differences. However, since the number of missing values was comparable in both groups, the statements on the group differences should not be distorted.
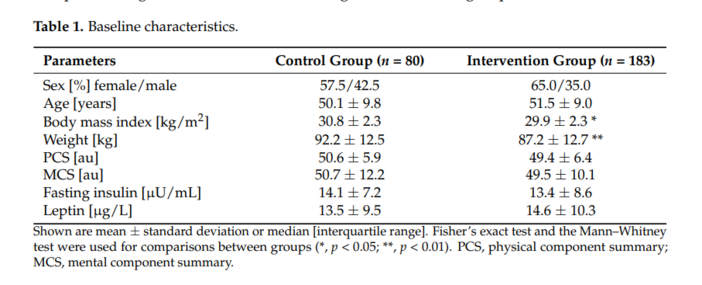
Higher values for BMI and weight have been observed in the control group. A higher BMI is usually associated with a lower HRQOL [16]. However, the baseline values for PCS and MCS were not statistically significantly different between the groups and rather showed a trend towards lower baseline values in the intervention group. It can therefore be assumed that the higher values for BMI and weight in the control group at baseline have not had any significant influence on the results.
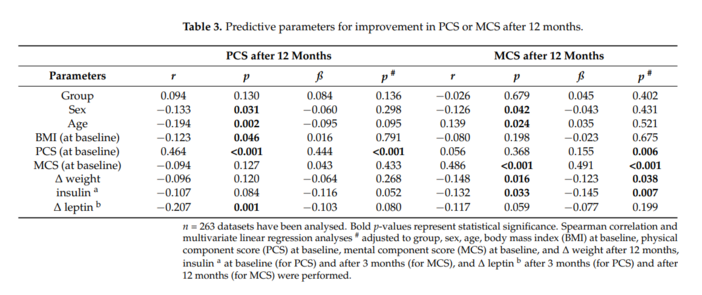
An additional bias might have occurred in the correlation analyses when the participants in the control and intervention groups were analysed together. However, this was due to the fact that the number of participants in separated groups would have been too small to be able to find statistically significant associations. In addition, this analysis was intended to examine general effects for which group membership plays a subordinate role. A strength of our work is that we analysed the influence of BMI and weight change in a multivariate regression model, along with other factors such as baseline PCS and MCS. Although the absolute values of PCS increased significantly only in the intervention group and a significant difference in the change in the PCS after 12 months has been observed between the groups, correlation analysis did not show a significant impact for group membership. This is explained by the fact that the absolute PCS level after 12 months was mainly dependent on the absolute PCS value at baseline, which tended to be slightly lower in the intervention group at baseline. Since, also, BMI has been shown to have a negative impact on HRQOL, it was rightly demanded [16] that these important parameters have to be taken into account when determining the effectiveness of an intervention.